While pregnant, a person’s risk for blood clots in their veins (venous thromboembolism) increases 5- to 6-fold. Homocysteine is a metabolic by-product. High homocysteine levels (hyperhomocysteinemia) can indicate a vitamin B12, B6, or folate deficiency, and is a risk factor for thrombosis and cardiovascular disease as well as adverse pregnancy outcomes.
Physiology
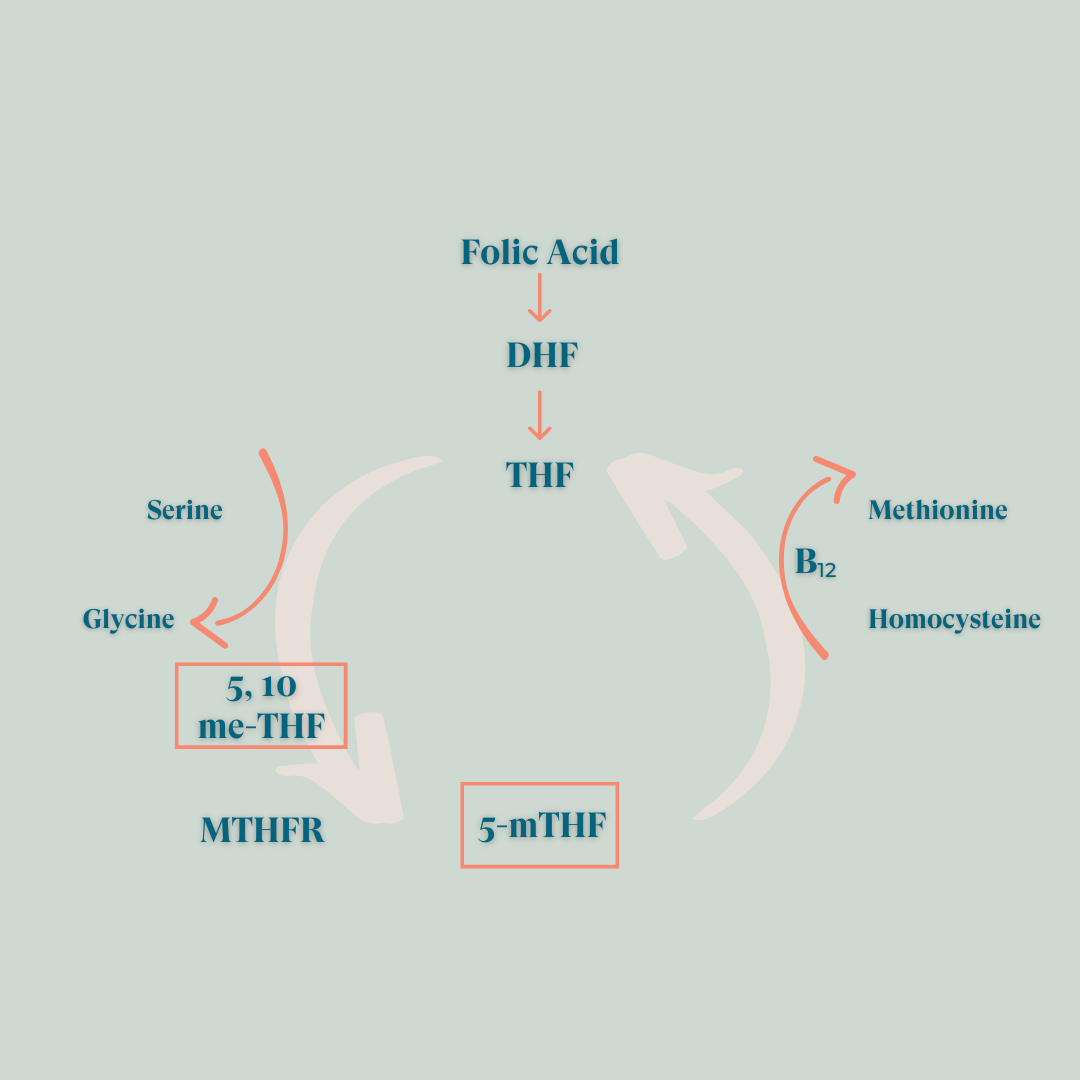
MTHFR (5, 10 methylenetetrahydrofolate reductase) is one of the key enzymes involved in folic acid metabolism and is directly responsible for homocysteine conversion to methionine (figure below). Folate and methionine are essential for nucleic acid synthesis (component of your DNA) and are required for methylation reactions.
Normal MTHFR activity is crucial to maintain normal levels of circulating folate and methionine and is key to prevent the accumulation of homocysteine.
Hyperhomocysteinemia is observed in approximately 5% of the general population and is associated with increased risk for many inflammatory disorders including auto immune disorders (Rheumatoid Arthritis, Diabetes, Multiple Sclerosis, Systemic Lupus erythematosus, Grave disease), birth defects and adverse pregnancy outcomes (pre-eclampsia, placental abruption, spontaneous abortion, low birth weight), as well as vascular and neurodegenerative diseases. Homocysteine is at the epicenter of oxidative stress and DNA methylation errors.
Published clinical data
Elevated serum homocysteine concentration is an important problem causing birth defects1, pre-eclampsia2-4, placental abruption2, low birth weight and other maternal or fetal complications5.
References
- Zhang Y, He X, Xiong X, Chuan J, Zhong L, Chen G, Yu D. The association between maternal methylenetetrahydrofolate reductase C677T and A1298C polymorphism and birth defects and adverse pregnancy outcomes. Prenat Diagn. 2019 Jan;39(1):3-9.
- Chaudhry SH, Taljaard M, MacFarlane AJ, Gaudet LM, Smith GN, Rodger M, Rennicks White R, Walker MC, Wen SW. The role of maternal homocysteine concentration in placenta-mediated complications: findings from the Ottawa and Kingston birth cohort. BMC Pregnancy Childbirth. 2019 Feb 19;19(1):75.
- Brenner B, Aharon A. Thrombophilia and adverse pregnancy outcome. Clin Perinatol. 2007 Dec; 34(4):527-41, v. Review. PubMed PMID: 18063103.
- Den Heijer M, Koster T, Blom HJ, Bos GMJ, Briët E, Reitsma PH, Vandenbroucke JP, Rosendaal FR. Hyperhomocysteinemia as a risk factor for deep-vein thrombosis. N Engl J Med. 334, 1996, 759-762.
- Enciso M, Sarasa J, Xanthopoulou L, Bristow S, Bowles M, Fragouli E, Delhanty J, Wells D. Polymorphisms in the MTHFR gene influence embryo viability and the incidence of aneuploidy. Hum Genet. 2016 May;135(5):555-68.
More to read
- Research Antinuclear Antibodies and Pregnancy: Research Review
- Research Blood Clotting and Pregnancy
- Research Autoimmune Disease Predispositions and Pregnancy
- Fertility National Infertility Awareness Week
- Fertility Polycystic Ovarian Syndrome (PCOS) and Fertility
- Research PAI-1, Thrombophilia and Pregnancy: Research Review